As a new mom, the “breast is best” message hits you loud and clear from all sides — health experts, friends, family, and random strangers. Breastfeeding is framed as the single most important thing a mother can do for her child.
Depending on who you ask, breastfeeding promises to deliver everything from fewer childhood infections, to lower rates of obesity, diabetes, cancer and asthma, to higher IQ. To cash in on these benefits, we are advised to exclusively breastfeed for 6 months, and to continue up to a year or longer.
See the breastfeeding guidelines and benefits promoted by the American Academy of Pediatrics, Health Canada, & World Health Organization.

Many moms take this panacea portrayal to heart. It drives them to pursue breastmilk at all costs, making steep personal sacrifices, like spending inordinate amounts of time hooked up to a breast pump. It also provokes a lot of grief and guilt in those who don’t or can’t exclusively breastfeed. I would know. I’ve been there.
I feel strongly that all parents deserve a more rigorous look at the science behind breastfeeding benefits so that they can make informed choices rooted in accurate information. Those for whom breastfeeding is not a viable option also deserve to know the truth.
Is breastfeeding really a golden ticket to lifelong health and success?
Before we dive in, let’s set the stage with a few insights into why the study of breastfeeding benefits isn’t straightforward.
Studying breastfeeding benefits
The first complicating factor in the study of breastfeeding is study design. Most of the evidence behind the claims we see comes from uncontrolled, observational studies (e.g. observational studies or case-control cohort). Such studies cannot tease apart correlation and causation.
The second complicating factor is a high risk of confounding. The women who aggressively pursue breastfeeding may differ in meaningful ways from those who don’t. For example, we tend to see breastfeeding rates rise with education and income (see Health Canada data).
Thus, when we observe differences between babies of women who breastfeed and those who don’t, we can’t always attribute them to the milk. If the study wasn’t fully controlled, those differences may reflect other advantages that mothers brought to the table. You can try to use statistics to correct for these “confounders” — like education, income, and BMI — but such measures are never perfect.
To truly establish causation, we need rigorously controlled trials like randomized controlled trials (RCTs) and sibling comparisons. Such trials truly eliminate the effect of confounders. In the world of breastfeeding, these studies are few and far between, for ethical and cost reasons. When we zero in on them, the list of benefits shrinks massively, as do the effect sizes.
The discussion below focuses on what we’ve learned from a few uniquely well-controlled studies, including the PROBIT RCT in Belarus (over 17,000 women), and a collection of sibling studies in the United States.
To be clear, I’m not saying we need to throw out the hundreds of less rigorous studies out there. We can still learn from observational and case-control cohort studies, especially when we have a large, diverse, collection. However, we need to acknowledge their caveats and adjust our messages when they are refuted by controlled trials. This nuance is missing from the breastfeeding narrative.
What happens when we raise the scientific bar?
Short Term Impact
- Breastfed infants are less likely to experience gastrointestinal GI infections (e.g. diarrhea), eczema and other rashes.
- Breastmilk may offer some protection against a serious condition called Necrotizing Enterocolitis (NEC) to preterm low birthweight infants.
- Breastfeeding may help protect against ear infections, but effects are moderate at best. Protection was not significant according to the PROBIT study but a large, well-designed cohort study supported a small benefit.
- It’s unclear whether or not breastfeeding helps reduce rates of Sudden Infant Death Syndrome (SIDS). The PROBIT trial did not find statistically significant differences in SIDS rates between the two study groups, despite numbers that favoured breastfeeding. Case-control studies provide some support for lower rates of SIDS with breastfeeding, but the link is murky. This 2017 review of eight international case-control studies didn’t show protective effect in the first 2 months, either in individual studies or the pooled analysis. From 2–6 months, some studies showed a protective effect of breastfeeding, while others didn’t. The pooled analysis landed in support of breastfeeding protection, though there was no difference between exclusive breastfeeding and some breastfeeding. There is no clear mechanism for how breastfeeding helps.
Sudden Infant Death Syndrome. Learn more about SIDS risk factors and what you can do to modify risk, like quitting smoking and encouraging them to sleep on their backs.
- In the developed world, there does not appear to be a link between breastfeeding rates and overall infant mortality. The PROBIT RCT did not find significant differences in overall infant death rates between the breastfeeding intervention group and the control group (2.3 deaths vs 3.7 per 1000 live births). Similarly, this 2007 review examined a large collection of mostly uncontrolled studies and did not find a link between breastfeeding and overall infant mortality in developed countries (as discussed below, the story is different in the developing world).
- Many other short term benefits (e.g coughs and colds) lack rigorous evidence.
Long Term Impact
Most claims of long term benefits to breastfeeding, such as childhood obesity, asthma, and intelligence, are not supported by well-controlled trials.
Skeptical? I highly recommend checking out this enlightening 2014 study entitled: “Is breast truly best? Estimating the effects of breastfeeding on long-term child health and wellbeing in the United States using sibling comparisons”. They examined 11 outcomes (e.g. BMI, obesity, asthma, hyperactivity, parental attachment, and various academic measures) in children aged 4–14 and found that none of them were supported by the data. The study also demonstrated how the same data yielded a different answer (in support of breastfeeding) when all subjects were lumped together without factoring the households they came from.
According to study leads Colen and Ramey:
Our results suggest that much of the beneficial long-term effects typically attributed to breastfeeding, per se, may primarily be due to selection pressures into infant feeding practices along key demographic characteristics such as race and socioeconomic status.
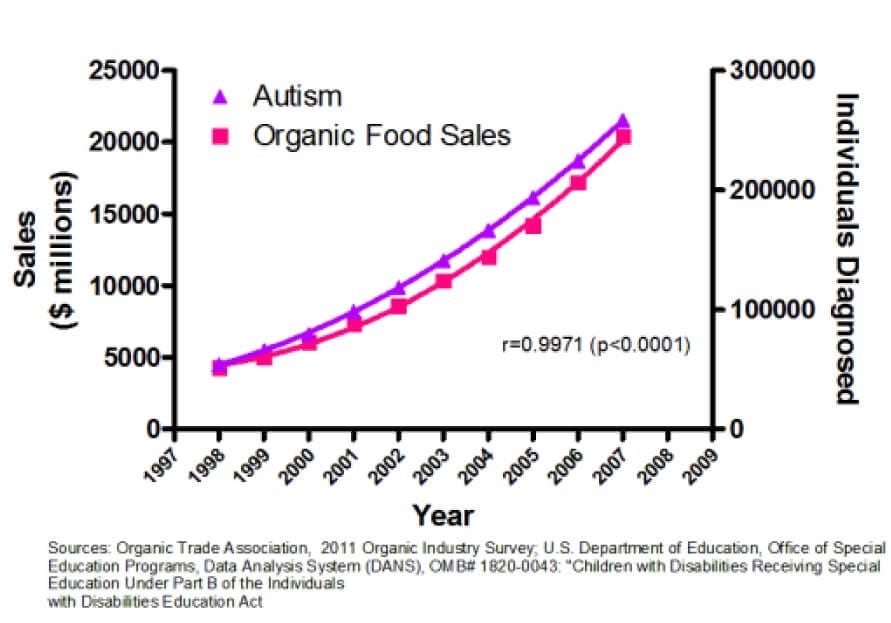
In other words, we are inferring causation when all we have is a correlation — just like the false link between autism and organic food sales (a graph made in jest, to illustrate the point).
What about moms?
Moms may also benefit health-wise from breastfeeding, but the story here is also more complex than meets the eye, as described in this 2015 maternal health review. As with infant benefits, most of the evidence comes from uncontrolled studies that make it difficult to draw firm causal conclusions.
When we raise the scientific bar, we get good and bad news.
The good news is that there is fairly strong evidence for a reduced risk of breast and ovarian cancers. These claims also have biologically plausible mechanisms. Yet, even these benefits are not straightforward. For example, the massive US Nurses Health study, failed to find a protective effect of breastfeeding on breast cancer risk. Some of this inconsistency likely reflects the fact that the terms “breast cancer” and “ovarian cancer” actually encompass several distinct diseases with different causes, treatments, and outcomes. Yet, many studies treat breast and ovarian cancers as if they were each a single disease.
As someone with expertise in cancer research, viewing all breast cancers as a single disease makes as much sense to me as lumping together breast cancer and lung cancer!
More good news: concerns of meaningful bone density loss due to breastfeeding are not consistently supported across studies.
The not-so-great news is that there is no guarantee that breastfeeding will get provide greater postpartum weight loss.
More Nuance
It’s important to distinguish between “formula is bad” (false) and “breast milk is extra special” (true). The well-supported differences between breast and formula fed infants stem largely from the immune boosting factors uniquely found in breast milk (e.g. antibodies), not from formula being harmful.
The differences between breast versus formula depend a lot on global context. Breastmilk far more significant advantages in developed countries without access to clean water, and where protection from antibodies contained in breast milk play a more meaningful role in infant health. Diarrhea, for example, is usually not much more than a nuisance in the developed world, but can be lethal in poor countries. Developing countries also face a battle against misinformation falsely promoting formula as superior to breastmilk.
The cost of exaggeration
Some breastfeeding advocates seem to feel that a little exaggeration can only help, by nudging moms towards the “right” track. I disagree.

Preaching exaggerated benefits of breastfeeding, while implying that formula is evil, is far from harmless. In its most extreme form, “lactivism” — the doctrine or practice of extreme actions as a means of achieving a breastfeeding culture — can be downright toxic (check out Lactivism by Courtney Jung).
It fails to account for the wellbeing of mothers, who are being told to bear any personal cost, no matter how steep. It also ignores the mental toll for those for whom this path isn’t available, or who choose otherwise. Feelings associated with the inability to breastfeed may even contribute to suicide in new mothers suffering from postpartum depression (see Florence Leung’s story, a local mom).
For me, these issues are not just theoretical. I’ve felt the shame, guilt, and judgment for being unable to exclusively breastfeed my three children, despite my best efforts.
The path forward
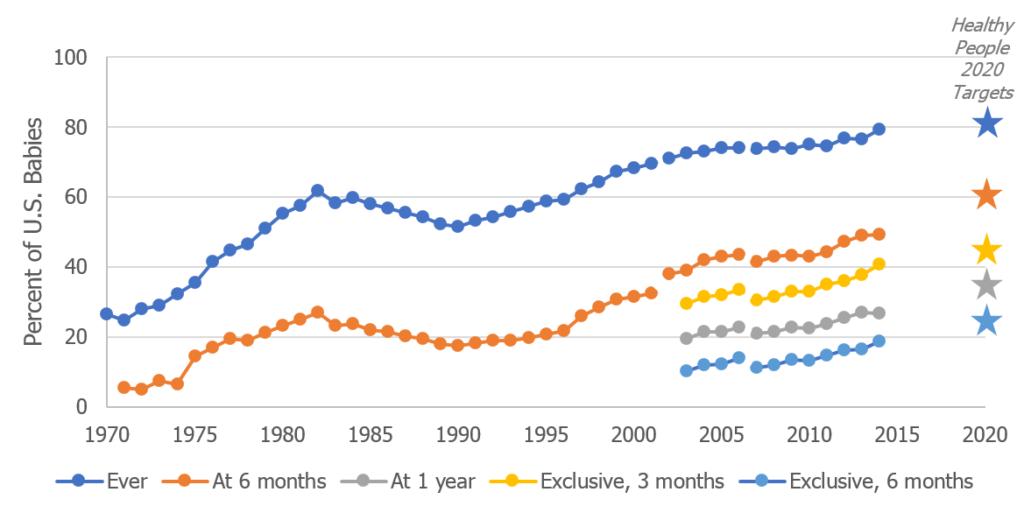
In theory, greater rates of breastfeeding would be a boon both to babies, moms, and public health systems. Breastfeeding rates still have a lot of room to grow since their dramatic drop following World War II.
Are breastfeeding rates hampered by a perceived lack of value?
Here in North America, the numbers suggest otherwise. Most women do try breastfeeding— nearly 9 of 10 mothers in Canada, and just over 8 of 10 moms in the United States. Yet, they struggle to stick with it, and few attain the recommended 6 months of exclusivity.
Is trumpeting a longer list of benefits really going to help?
It seems to me that the real issue with breastfeeding in developed countries is lack of support for parents. I’d love to see more lactation support, better job and income security, and more support from society at large. While I’m on my soapbox, I’d also like to pound the table for access to accurate information that allows parents to make truly informed choices.
We can also do a better job of supporting each other. We can share our candid, raw new mom stories (read mine here), and stop judging others who make different choices. We can give ourselves permission to factor our own wellness into the equation, and let go of our mommy guilt.
My Bottom Line
Breastfeeding does offers real short term health advantages, both for babies and moms. Yet, the differences between breastfed and bottle fed babies aren’t nearly as dramatic as they are made out to be.
Breastmilk won’t make or break your child’s future. It’s not the single most important decision you will ever make. It doesn’t define your ability to be a good mother.
If it fits you, and your life, breastfeeding can be a wonderful win-win. If not, please don’t feel racked with guilt.
Advertising an inflated, purist view can do as much harm as good. We parents deserve more balance, more nuance, and more rigour.
Credit
Thank you, SciMoms and Prof. Emily Oster whose work on this topic inspired and informed this article and my own deep dive.